


We need to fix the Multi-Disciplinary Team (MDT) meeting problem
Without the right technical support, Multi-Disciplinary Team (MDT) meetings could stop working to the patients' advantage

1.
It is now ten years since the surgeon Ian Paterson— the infamous butcher of Solihull— was suspended from medical practice; four and a half years since he was jailed; and nearly two years since the Paterson Enquiry published its report. A few days ago Paterson was refused the legal opportunity to challenge his convictions.
In all that time, many things have changed for the better. In my work improving safety in hospitals in both the UK and China I have noticed an increased willingness to challenge healthcare colleagues – including senior doctors – in order to protect patients from preventable harm.
Trust-level boards in the NHS have also tightened their governance structures – and the appraisal system for doctors has become further embedded. But Ian Kennedy, the author of the first Kennedy review, in 2013 wrote in early 2020 that there remain stubborn and difficult cultural and political problems throughout the NHS – implying that a similar tragedy could still be happening somewhere in the UK health system.
The recommendations of both reports concentrated rightly on the need for cultural and systemic changes at board and trust-leadership level. The Patterson report also make specific the need for better compliance with standards of Multi-Disciplinary Teams Meetings (MDTMs). It said:
We recommend that CQC, as a matter of urgency, should assure itself that all hospital providers are complying effectively with up-to-date national guidance on MDT meetings, including in breast cancer care, and that patients are not at risk of harm due to non-compliance in this area.
The guidance at the time was from 2019 that emphasised streamlining. The guidance also assumed that the MDTMs should be held as a single meeting, with the whole team in attendance.
But a consequence of these recommendation has been an increased number of Multi-Disciplinary Teams (MDTs) to cover many of other challenging clinical decisions.
The CQC inspection framework (most recently updated in 2020) added several more references to MDTs and included the need for one during End of Life Care (page 16), weekly MDTs for people with complex needs (page 36); and also mentions ‘Tumour MDTs” – not just breast cancer (page 37) – which seems to imply all tumours (although I’m not clear if this include benign growths).
A serious problem with this proliferation is lack of time and availability of staff to attend these meetings in one place, at one time. Admittedly videoconferencing has improved rapidly since the start of the pandemic, but this is still a lot of meetings. And we all know that meetings can be tiresome, inefficient and – in Paterson’s case – fraught and counter-productive.
Aside from the problem with time, an additional problem is available competency, especially for smaller providers in the independent sector (and that would include the two independent hospitals in which Paterson worked). Independent hospital MDTs, where a lot of the NHS recovery work will no doubt be done, are hard to staff unless the hospital has good relations with their local trust or larger provider.
The consequence of this is that the effectiveness of Multi-Disciplinary Teams (MDTs) is under increasing pressure and is already seeing an erosion of their power to assure safe can appropriate care. Anecdotally, I have been told that the increasing burden of MDTs mean that non-compliance (primarily non-attendance by key members) is a significant quality issue for many hospitals. This is not a problem of engagement — all MDT members want to, and are willing to provide input — but staffing pressures and the complexity of rostering makes holding these meetings near-impossible.
So how do we stop this degradation and better manage the burgeoning number of MDTs?
One possible answer is to change the emphasis from a single meeting to a managed series of recorded opinions and decisions. If properly supported by the right workflow technology, we can move away from the ‘single-point’ MDT meeting (MDTM) to a ‘multi-point’ MDT process (MDTP) which could allow better and more auditable decisions to be made. Where significant differences of opinion exist, then a meeting can be called – but the Multi-Disciplinary Team (MDT) members could act independently and in parallel using a suitable recording and monitoring system.
It would then not be a huge or time-consuming step to include outcome data against these decisions, and thereby provide the feedback that would allow MDT decisions to improve and learn from experience.
2.
How exactly might that work? My answer is to support an asynchronous process using an online system, that allows MDT members to provide their opinions individually and collate these.
Full disclosure: I am the CEO of a company that makes software — the CAREFUL platform— that could provide the technological support for this. What follows includes a discussion of such a process. .
An MDT Process
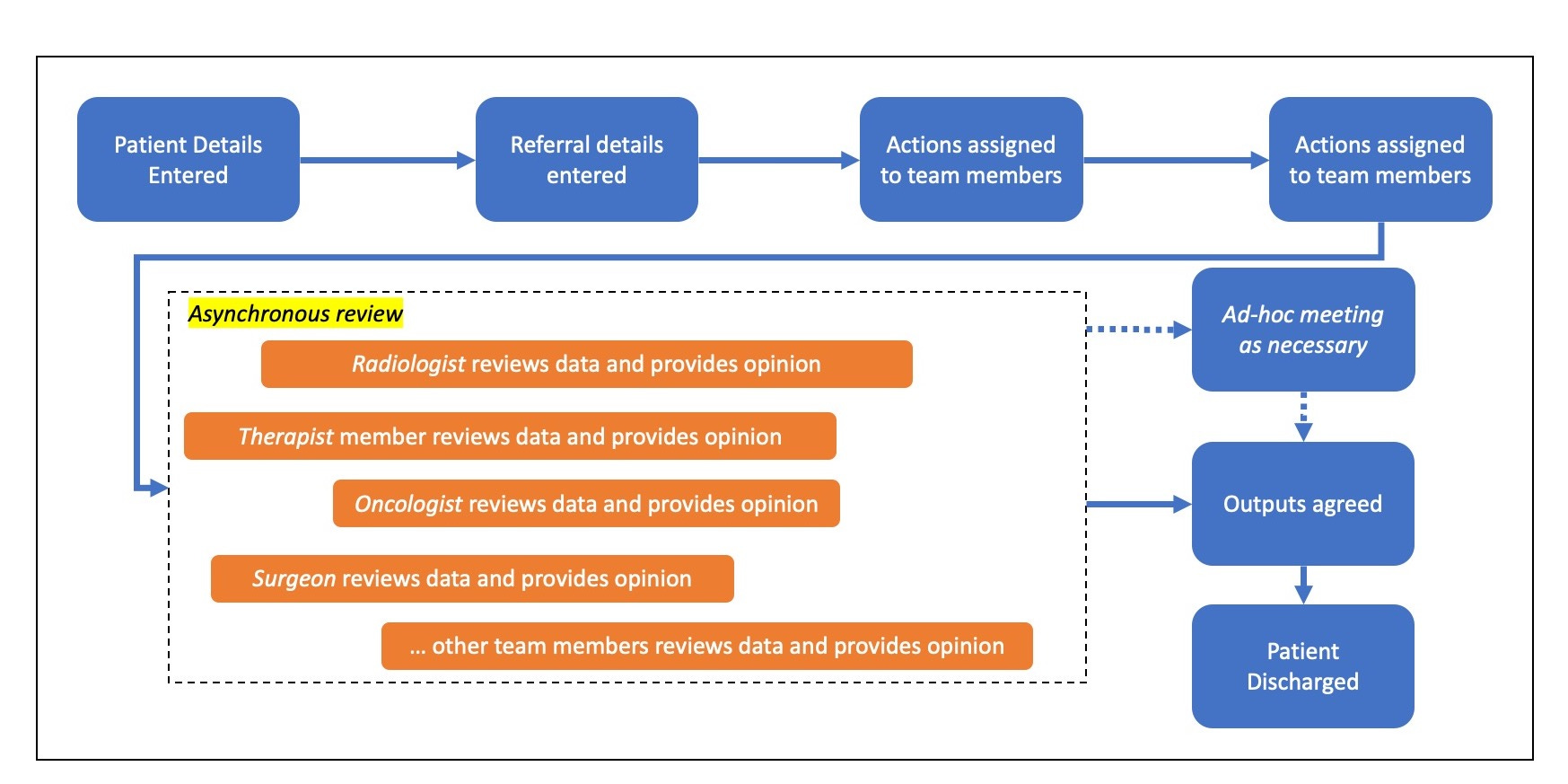
Here is an outline of an MDT process
A patient is crated in a dedicated, secure MDT patient list (could be ‘sent’ from or looked-up in an EPR, or manually entered).
Required referral summary uploaded to a secure patient-specific document storage area. This includes expected or planned treatment or questions to be answers.
Supporting documents (e.g. scans, letters, other notes) are uploaded to the same location
Actions are assigned to relevant members of the Multi-Disciplinary Team (MDT), requesting their opinion on the case.
Documents are reviewed by each member of the Multi-Disciplinary Team (MTD), in their own time, who provide written summaries of their opinion.
If the result is equivocal, then an ad-hoc meeting is called for detailed discussion.
Summary output information is entered into the system.
The result of this is then agreed by the Multi-Disciplinary Team (MDT) leader, printed out or emailed back to the referrer.
The patient is discharged from the team
{kind=link}
The advantages of this system, f all user activity within the system is automatically logged, then this will provide an audit-trail identifying how the decision was reached and can be printed for the patient’s notes or for subsequent investigation should one be needed.
Patients can also be referred in this system to non-MDT teams such as quality teams who can monitor compliance and enter PROMS or other outcome data against the patient.
Finally, using such a system in place, MDT activity could be batched by individuals, making their life easier and more efficient.
This could, very possibly, provide a way of resisting the bullying tactics used by Patterson all those years ago.